🇬🇧🇮🇹 Vincenzo is a Christian, a husband, a dad, a theologian, an apologist, a scientist, a polyglot, and an anglicised Neapolitan. Not always in this order.
The PCR test “is unable to determine, beyond reasonable doubt, that a positive result corresponds, in fact, to the infection of a person by the SARS-CoV-2 virus”, said the Lisbon Court of Appeal.
Mass PCR testing is creating a casedemic, that is, a pandemic of allegedly Covid-positive people, the overwhelming majority of which isn’t actually ill.
There are four main factors contributing to poor performance of PCR testing:
1. Low prevalence of disease. This is the case in the UK and most of Europe. «When virus levels in the population are very low, the chances of a test accurately detecting Covid-19 could be even less than 50 per cent»
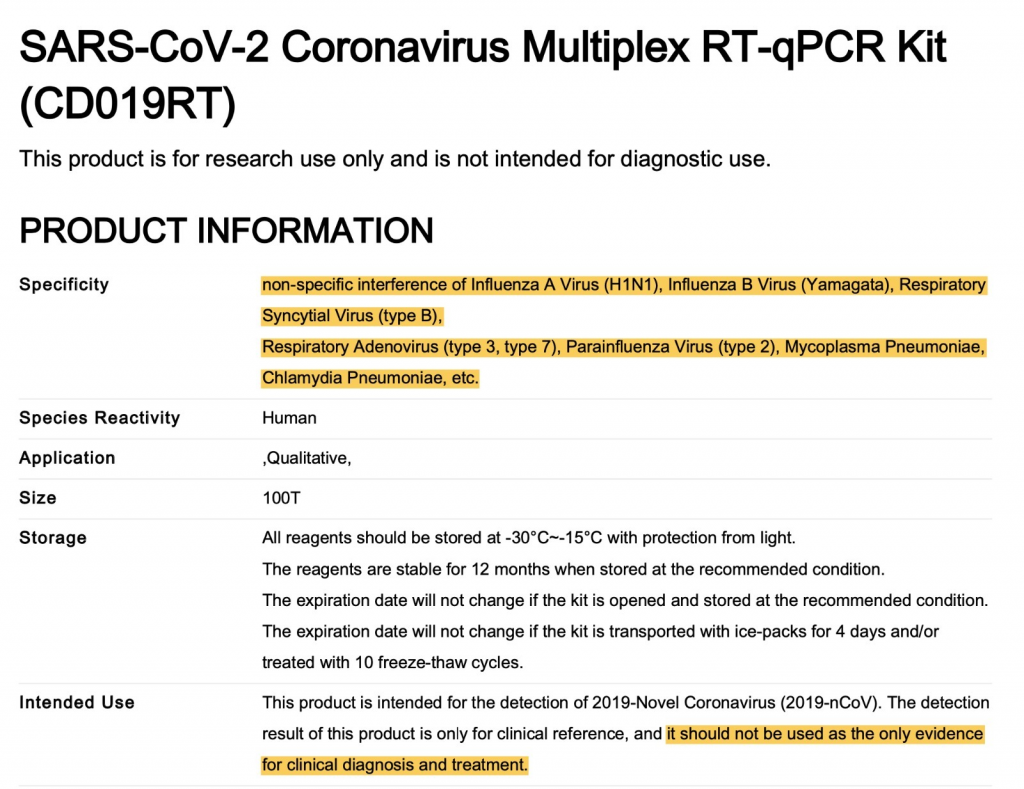
2. High cycle threshold. The PCR test amplifies genetic matter from the virus in cycles; the fewer cycles required, the greater the amount of virus, or viral load, in the sample. The greater the viral load, the more likely the patient is to be contagious. This number of amplification cycles needed to find the virus, called the cycle threshold, is never included in the results sent to doctors and coronavirus patients, although it could tell them how infectious the patients are. Any test with a cycle threshold above 35 is too sensitive, and yet most Covid-19 tests have a CT of 40, with some with a CT as high as 47, and just few with a CT of 37. In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle threshold of 40 would have been deemed negative if the threshold were 30 cycles. This was observed and published about already in May: Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic Samples.
3. Cross T-cell immunity. There’s mounting evidence of cross T-cell immunity for coronaviruses, meaning that even exposure to common cold viruses (these, too, are coronaviruses) trains the immune system to respond to more dangerous coronaviruses (SARS 1 and 2, MERS). See, amongst others:
4. Lack of specific RNA sequences required by testing.There is no guidance providing details on the specific RNA sequences required by testing, a threshold for the test result and the need for confirmatory testing. It is therefore not clear what constitutes a positive result.
All this is creating a wave of cases, which in most part are people who are not actually sick. The pandemic seems to be over, and it also seems that many don’t want it to be.
This is clear from WHO guidance on what constitutes a positive case, which are pretty much followed in most of the western world:
A suspect case has clinical symptoms of respiratory disease, perhaps with other associated presentations.
A probable case is a suspect case for whom laboratory testing was inconclusive or not possible.
A confirmed case is “A person with laboratory confirmation of COVID-19 infection, irrespective of clinical signs and symptoms.”
Notice how suspect and probable rely on a broader clinical picture, whereas the confirmed relies solely on the PCR test, irrespective of clinical signs and symptoms.This is very bad, since asymptomatic people are by and large not actually ill. This is why:
The one thing historically people need to realise [is] that even if there is some asymptomatic transmission, in all the history of respiratory-borne viruses of any type, asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is always a symptomatic person. Even if there is a rare asymptomatic person that might transmit, an epidemic is not driven by asymptomatic carriers.
Dr ANthony Fauci
BOOM! Right from the Infectious Disease God himself. Game over.
Symptomatics transfer. Not Asymptomatic.
Asymptomatic transmission of Covid is a non issue. The story had to be made up so pharma could save the day with another vaccine nightmare pic.twitter.com/eZ9DFC5Bg8
Remember (probably not) when I made a big fuss about PCR tests being unreliable? Many back then, even amongst friends and such, told me: “you are conspiracy guy — do you know better than doctors?”.
Well, it turns out I was right (every person of sane mind knew that, anyway): CDC to withdraw current tests, which are to be replaced with new ones able to tell Covid from Flu.
I’ve written already on why there is abundant reason not to trust PCRs for diagnosis of the pandemic status of SARS-CoV-2. I’ve added that over-reliance on these methods can easily lead to psuedo-epidemics.
This time I want to present you with other factual sources on PCR.
RT-PCR tests can detect viral SARS-CoV-2 RNA in the upper respiratory tract for a mean of 17 days; however, detection of viral RNA does not necessarily equate to infectiousness, and viral culture from PCR positive upper respiratory tract samples has been rarely positive beyond nine days of illness.
A PCR test might find the virus it was looking for. This results in a PCR positive, but a crucial question remains: is this virus active, i.e. infectious, or virulent? The PCR alone cannot answer this question. The CEBM explains why culturing the virus is needed to answer this question:
“In viral culture, viruses are injected in the laboratory cell lines to see if they cause cell damage and death, thus releasing a whole set of new viruses that can go on to infect other cells.”
there is no guidance providing details on the specific RNA sequences required by testing, a threshold for the test result and the need for confirmatory testing. It is therefore not clear to us what constitutes a positive result
— Read on www.cebm.net/covid-19/when-is-covid-covid/
PCR tests are picking up rubbish. Literally. They are picking up “dead virus” so to speak, that is, incomplete viral genome that doesn’t make anybody sick.
Coronavirus cases are mounting but deaths remain stable. Why? Evidence is mounting that a good proportion of ‘new’ mild cases and people re-testing positives after quarantine or discharge from hospital are not infectious, but are simply clearing harmless virus particles which their immune system has efficiently dealt with.
Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be. In three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to 90 percent of people testing positive carried barely any virus, a review by The Times found. […] In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle threshold of 40 would have been deemed negative if the threshold were 30 cycles, Dr. Mina said. “I would say that none of those people should be contact-traced, not one,” he said.
Warum alle falsch lagen (English translation: Why everyone was wrong). Even if the infectious viruses are long dead, a corona test can come back positive, because the PCR method multiplies even a tiny fraction of the viral genetic material enough [to be detected]. That’s exactly what happened, when there was the global news, even shared by the WHO, that 200 Koreans who already went through Covid-19 were infected a second time and that there was therefore probably no immunity against this virus. The explanation of what really happened and an apology came only later, when it was clear that the immune Koreans were perfectly healthy and only had a short battle with the virus. The crux was that the virus debris registered with the overly sensitive test and therefore came back as “positive”. It is likely that a large number of the daily reported infection numbers are purely due to viral debris. The PCR test with its extreme sensitivity was initially perfect to find out where the virus could be. But this test can not identify whether the virus is still alive, i.e. still infectous.
Preclinical studies of COVID-19 mRNA vaccine BNT162b2, developed by Pfizer and BioNTech, showed reversible hepatic effects in animals that received the BNT162b2 injection. Furthermore, a recent study showed that SARS-CoV-2 RNA can be reverse-transcribed and integrated into the genome of human cells. In this study, we investigated the effect of BNT162b2 on the human liver cell line Huh7 in vitro. Huh7 cells were exposed to BNT162b2, and quantitative PCR was performed on RNA extracted from the cells. We detected high levels of BNT162b2 in Huh7 cells and changes in gene expression of long interspersed nuclear element-1 (LINE-1), which is an endogenous reverse transcriptase. Immunohistochemistry using antibody binding to LINE-1 open reading frame-1 RNA-binding protein (ORFp1) on Huh7 cells treated with BNT162b2 indicated increased nucleus distribution of LINE-1. PCR on genomic DNA of Huh7 cells exposed to BNT162b2 amplified the DNA sequence unique to BNT162b2. Our results indicate a fast up-take of BNT162b2 into human liver cell line Huh7, leading to changes in LINE-1 expression and distribution. We also show that BNT162b2 mRNA is reverse transcribed intracellularly into DNA in as fast as 6 h upon BNT162b2 exposure.
— Read on www.mdpi.com/1467-3045/44/3/73
“We also show that BNT162b2 #mRNA is reverse transcribed intracellularly into #DNA in as fast as 6 h upon #BNT162b2 exposure.”
Healthcare workers (HCWs) are vulnerable to getting infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Preventing HCWs from getting infected is a priority to maintain healthcare services. The therapeutic and preventive role of ivermectin in coronavirus disease 2019 (COVID-19) is being investigated. Based on promising results of in vitro studies of oral ivermectin, this study was conducted with the aim to demonstrate the prophylactic role of oral ivermectin in preventing SARS-CoV-2 infection among HCWs at the All India Institute of Medical Sciences (AIIMS) Bhubaneswar.
Methods
A prospective cohort study was conducted at AIIMS Bhubaneswar, which has been providing both COVID and non-COVID care since March 2020. All employees and students of the institute who provided written informed consent participated in the study. The uptake of two doses of oral ivermectin (300 μg/kg/dose at a gap of 72 hours) was considered as exposure. The primary outcome of the study was COVID-19 infection in the following month of ivermectin consumption, diagnosed as per Government of India testing criteria (real-time reverse transcriptase polymerase chain reaction [RT-PCR]) guidelines. The log-binomial model was used to estimate adjusted relative risk (ARR), and the Kaplan-Meier failure plot was used to estimate the probability of COVID-19 infection with follow-up time.
Results
Of 3892 employees, 3532 (90.8%) participated in the study. The ivermectin uptake was 62.5% and 5.3% for two doses and single dose, respectively. Participants who took ivermectin prophylaxis had a lower risk of getting symptoms suggestive of SARS-CoV-2 infection (6% vs 15%). HCWs who had taken two doses of oral ivermectin had a significantly lower risk of contracting COVID-19 infection during the following month (ARR 0.17; 95% CI, 0.12-0.23). Females had a lower risk of contracting COVID-19 than males (ARR 0.70; 95% CI, 0.52-0.93). The absolute risk reduction of SARS-CoV-2 infection was 9.7%. Only 1.8% of the participants reported adverse events, which were mild and self-limiting.
Conclusion
Two doses of oral ivermectin (300 μg/kg/dose given 72 hours apart) as chemoprophylaxis among HCWs reduced the risk of COVID-19 infection by 83% in the following month. Safe, effective, and low-cost chemoprophylaxis has relevance in the containment of pandemic alongside vaccine.
In meno di 48 ore dall’insediamento ufficiale del cavallo di Troia Cinese, Joe Biden, ecco cosa succede in merito alla questione Covid-19:
OMS pubblica linee guida aggiornante riguardo i test PCR (“tamponi molecolari” come vengono chiamati in Italia). E all’improvviso OMS dice le stesse cose che migliaia di scienziati hanno denunciato in tutto il mondo da Aprile scorso:
Bisogna usare una CT più bassa, perché troppo alta provoca falsi positivi (ma dai?)
Se il test risulta positivo ma il quadro clinico della persona non combacia, bisogna testare di nuovo la persona, con lo stesso test o uno diverso. In altre parole: una persona asintomatica se è positiva non va considerata malata. Anche questo si sapeva.
PCR sono stati declassati ad “aiuto per la diagnosi” (in realtà non sono affatto un metodo diagnostico), quindi vanno considerati tutta una serie di altri fattori (timing of sampling, specimen type, assay specifics, clinical observations, patient history, confirmed status of any contacts, and epidemiological information). Anche questa è pratica normale, e invece finora la linea guida era “PCR positivo? Contate un nuovo caso”.
Inoltre, i vari numeri usati per il terrorismo psicologico iniziano a scendere.
Ma, a livello italiano, la cosa più scioccante e vedere una televisione nazionale riportare l’incostituzionalità dello stato di emergenza e dei DPCM (cosa anche questa già risaputa; vedere qui, qui e qui):
Un servizio su una TV Nazionale parla dell' Illegittimità dei DPCM e insinua anche una volontà di stampo dittatoriale. Finalmente era anche ora! 😱 pic.twitter.com/adSfJt0c64
In pratica, tutto quello per cui sono stato ampiamente attaccato, ridicolizzato, preso in giro e offeso, era vero. Ovviamente. Quando non si è controllati dalla propaganda e si riesce ad analizzare i fatti, è difficile sbagliarsi.