🇬🇧🇮🇹 Vincenzo is a Christian, a husband, a dad, a theologian, an apologist, a scientist, a polyglot, and an anglicised Neapolitan. Not always in this order.
For all those who like to dismiss papers when they are either not yet peer-reviewed or published on journals that are not exactly mainstream, here is a paper published in Nature:
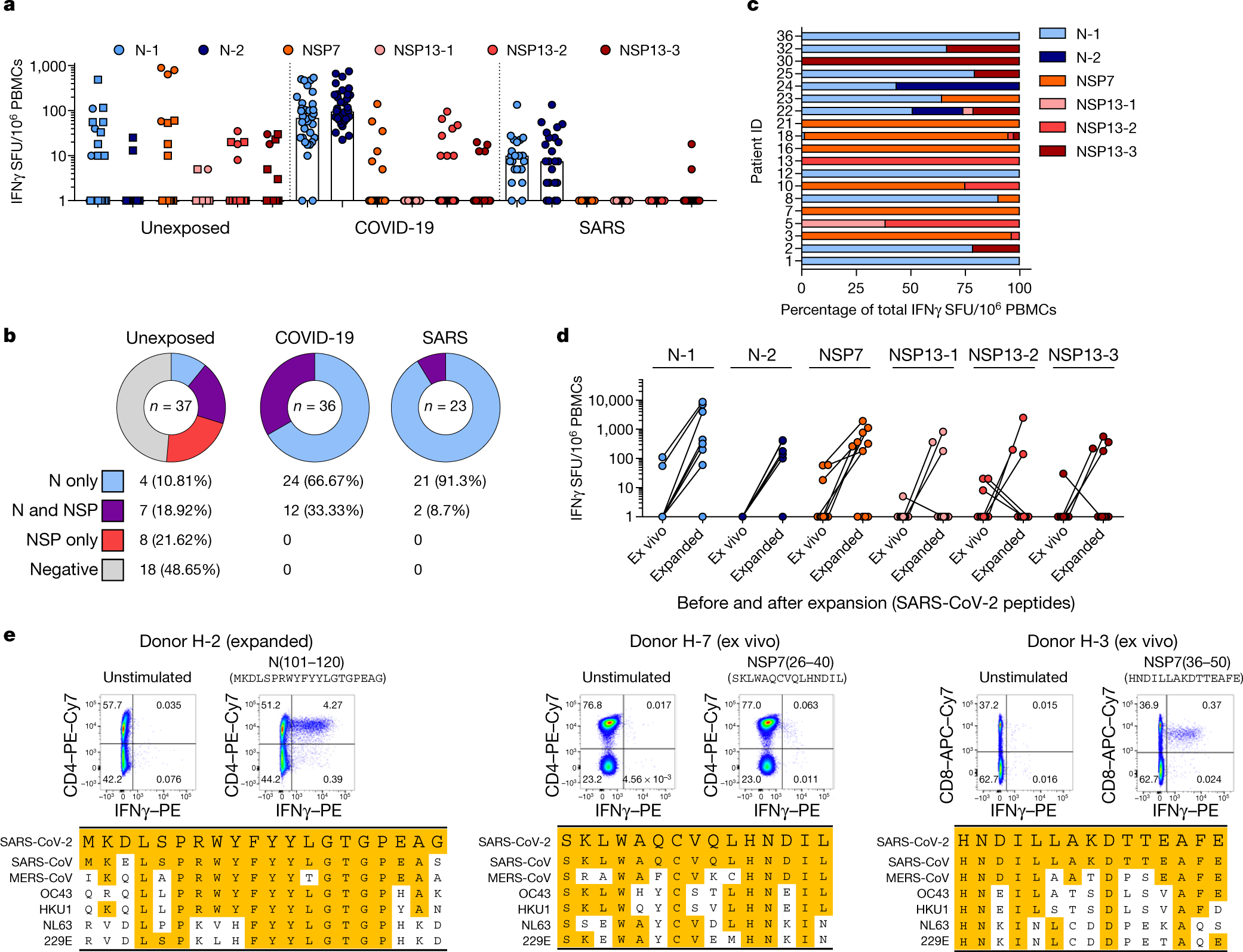
Covid-19 infection obviously creates T-cell immunity which long lasting and will protect people who recovered from ever getting Covid-19 again
People who caught SARS-CoV-1 (the first SARS) also have long lasting T-cell immunity (still working 17 years later) that works against Covid-19 (SARS-CoV-2)
Roughly 50% of the tested subjects who never caught either SARS viruses also had T-cell immunity that worked against Covid-19 due to a high degree of homology to the sequences of some proteins common to both SARS-CoV-2 and the common cold coronaviruses.
Mass PCR testing is creating a casedemic, that is, a pandemic of allegedly Covid-positive people, the overwhelming majority of which isn’t actually ill.
There are four main factors contributing to poor performance of PCR testing:
1. Low prevalence of disease. This is the case in the UK and most of Europe. «When virus levels in the population are very low, the chances of a test accurately detecting Covid-19 could be even less than 50 per cent»
2. High cycle threshold. The PCR test amplifies genetic matter from the virus in cycles; the fewer cycles required, the greater the amount of virus, or viral load, in the sample. The greater the viral load, the more likely the patient is to be contagious. This number of amplification cycles needed to find the virus, called the cycle threshold, is never included in the results sent to doctors and coronavirus patients, although it could tell them how infectious the patients are. Any test with a cycle threshold above 35 is too sensitive, and yet most Covid-19 tests have a CT of 40, with some with a CT as high as 47, and just few with a CT of 37. In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle threshold of 40 would have been deemed negative if the threshold were 30 cycles. This was observed and published about already in May: Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic Samples.
3. Cross T-cell immunity. There’s mounting evidence of cross T-cell immunity for coronaviruses, meaning that even exposure to common cold viruses (these, too, are coronaviruses) trains the immune system to respond to more dangerous coronaviruses (SARS 1 and 2, MERS). See, amongst others:
4. Lack of specific RNA sequences required by testing.There is no guidance providing details on the specific RNA sequences required by testing, a threshold for the test result and the need for confirmatory testing. It is therefore not clear what constitutes a positive result.
All this is creating a wave of cases, which in most part are people who are not actually sick. The pandemic seems to be over, and it also seems that many don’t want it to be.
This is clear from WHO guidance on what constitutes a positive case, which are pretty much followed in most of the western world:
A suspect case has clinical symptoms of respiratory disease, perhaps with other associated presentations.
A probable case is a suspect case for whom laboratory testing was inconclusive or not possible.
A confirmed case is “A person with laboratory confirmation of COVID-19 infection, irrespective of clinical signs and symptoms.”
Notice how suspect and probable rely on a broader clinical picture, whereas the confirmed relies solely on the PCR test, irrespective of clinical signs and symptoms.This is very bad, since asymptomatic people are by and large not actually ill. This is why:
The one thing historically people need to realise [is] that even if there is some asymptomatic transmission, in all the history of respiratory-borne viruses of any type, asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is always a symptomatic person. Even if there is a rare asymptomatic person that might transmit, an epidemic is not driven by asymptomatic carriers.
Dr ANthony Fauci
BOOM! Right from the Infectious Disease God himself. Game over.
Symptomatics transfer. Not Asymptomatic.
Asymptomatic transmission of Covid is a non issue. The story had to be made up so pharma could save the day with another vaccine nightmare pic.twitter.com/eZ9DFC5Bg8
there is no guidance providing details on the specific RNA sequences required by testing, a threshold for the test result and the need for confirmatory testing. It is therefore not clear to us what constitutes a positive result
— Read on www.cebm.net/covid-19/when-is-covid-covid/
PCR tests are picking up rubbish. Literally. They are picking up “dead virus” so to speak, that is, incomplete viral genome that doesn’t make anybody sick.
Coronavirus cases are mounting but deaths remain stable. Why? Evidence is mounting that a good proportion of ‘new’ mild cases and people re-testing positives after quarantine or discharge from hospital are not infectious, but are simply clearing harmless virus particles which their immune system has efficiently dealt with.
Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be. In three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to 90 percent of people testing positive carried barely any virus, a review by The Times found. […] In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle threshold of 40 would have been deemed negative if the threshold were 30 cycles, Dr. Mina said. “I would say that none of those people should be contact-traced, not one,” he said.
Warum alle falsch lagen (English translation: Why everyone was wrong). Even if the infectious viruses are long dead, a corona test can come back positive, because the PCR method multiplies even a tiny fraction of the viral genetic material enough [to be detected]. That’s exactly what happened, when there was the global news, even shared by the WHO, that 200 Koreans who already went through Covid-19 were infected a second time and that there was therefore probably no immunity against this virus. The explanation of what really happened and an apology came only later, when it was clear that the immune Koreans were perfectly healthy and only had a short battle with the virus. The crux was that the virus debris registered with the overly sensitive test and therefore came back as “positive”. It is likely that a large number of the daily reported infection numbers are purely due to viral debris. The PCR test with its extreme sensitivity was initially perfect to find out where the virus could be. But this test can not identify whether the virus is still alive, i.e. still infectous.
Part 1 of 4 of an interview with French professor, Christian Perronne. We hear about HCQ protocols, Ivermectin protocols, and also for the first time—at least for me—a clear explanation of the “Covid19 long haulers” mystery. If I got that right (I might have missed a few words when listening to French-accented English at 2x speed), what’s happening to long haulers is actually nothing new: some infections may lock a person’s immune system into a “poor state”, which means they start getting symptoms from a variety of germs and pathogens that are normally present in the environment and in a person’s body, but that would normally be kept in check by a healthy immune system. In essence, it’s a form of immunodeficiency that’s causing the long-lasting symptoms.
Professor Perronne has a long distinguished career in medicine. He was vice-chairman of the National Reference Centre on Tuberculosis and Mycobacteria at the Pasteur Institute in Paris. He is the past-president of the French College of Professors of Infectious and Tropical Diseases (CMIT). He was president of the Communicable diseases commission at France’s High Council for Public Health (HCSP), an official body making recommendations for public health and vaccination policies.
Since 1994, Professor Christian Perronne has been a leader in the the development of therapies for chronic Lyme disease, which brought him, well before COVID-19, to already challenge the medical establishment about how to treat this disease.
Professor Perronne has also considerable expertise with vaccination, as he is a past vice-president of the European Advisory Group of Experts on Immunisation – an official body advising the World Health Organization.
Professor Perronne was in the heat of the COVID-19 pandemic, as chief of a department of infectious diseases at the Raymond Poincaré University Hospital in Garches, belonging to the Greater Paris University Hospitals group. He used the therapeutic protocol developed in Marseille by Professor Raoult and his team, comprising hydroxychloroquine and azithromycin.
“COVID19 studies that have looked at very early outpatient treatment of high risk ppl, uniformly, every study shows the benefits of taking HCQ with.. AZM, Zinc.. when started in the first.. 5 days.”
Our whole society is politicized—unfortunately, science and medicine are no different. Mass media coverage is very one-sided: they do not cover any of the evidence showing that HCQ and Ivermectin work. They don’t cover the studies showing these drugs work.